
This guest post on selecting a diabetes medication was contributed by pharmacist Jiamin Liau who is also a Certified Diabetes Educator in Australia. I’m appreciative for her contribution to help educate other healthcare professionals! If you’re a pharmacist and have a case or scenario you’ve seen in your practice feel free to shoot me a message.
The past medical history of Mr. AD, 45 years old includes T2DM, hypertension, dyslipidemia, and stroke.
He was initiated on metformin XR 1000 mg twice daily nine months ago. Recent pathology results show HbA 1c 7.8% and eGFR 65 ml/min. His BMI is 29. Target HbA1c set for Mr. AD is 7%. If you were to add a second therapy to his current regimen, what oral agent would you choose?
A) Sulfonylureas
B) SGLT2 Inhibitors
C) DPP-4 Inhibitors
Sulfonylureas…is this a suitable add-on therapy for Mr. AD? Given that he has an elevated BMI and is relatively young, he may lead an active lifestyle. Sulfonylureas have a long track of record of success; they can, however, contribute to weight gain and may cause hypoglycemia. Cost considerations may also play a role in selecting this agent.
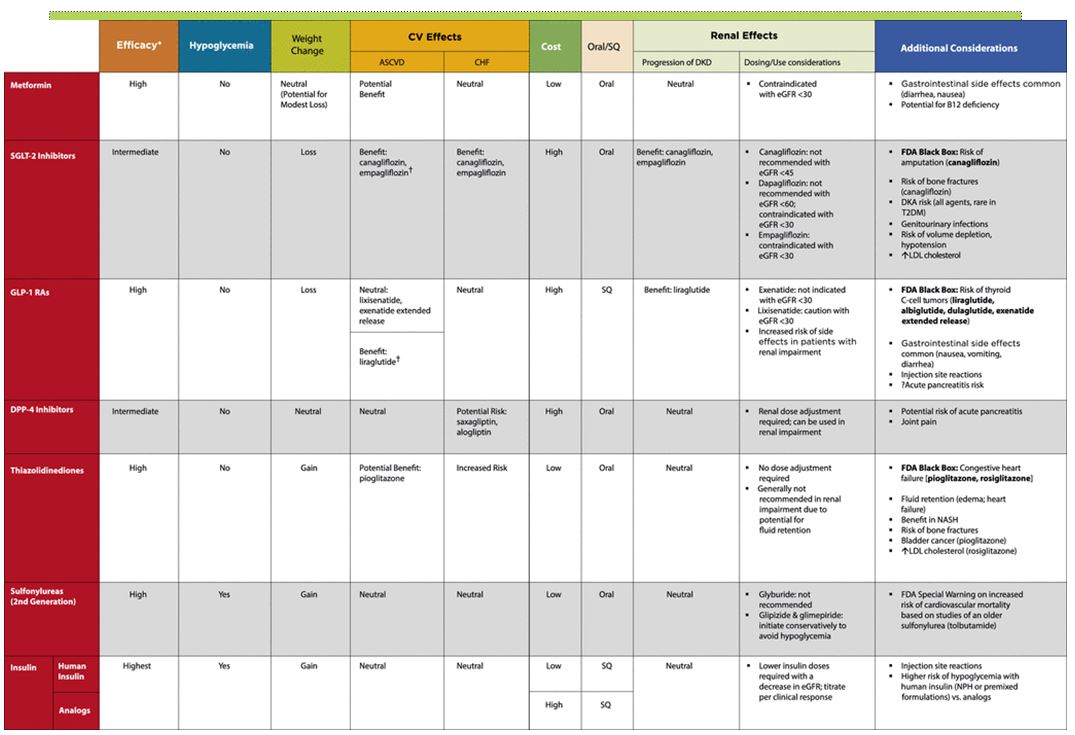
SGLT2 inhibitors inhibit a sodium-glucose cotransporter to induce urinary glucose loss and decrease blood sugar level. It has been shown to reduce HbA1c with no hypoglycemia, promote mild weight loss, CV protective effects (canagliflozin, empagliflozin) and renal protective effects (canagliflozin, empagliflozin).
On the other hand, the side effects of this medicine include dehydration and genitourinary infections. Should this be added to this existing therapy? If he is already receiving an ACE-inhibitor/ thiazide diuretic combination for his hypertension management, what are some additional counseling points to be included in his management plan?
Or should we consider a DPP-4 inhibitor for Mr. AD? DPP-4 inhibitors decrease inactivation of GLP-1 thereby increasing its availability (GLP-1 stimulates beta cell insulin release). DPP-4 inhibitors have weight neutral effect and do not cause hypoglycemia. Nonetheless, DPP-4 inhibitors can rarely cause acute pancreatitis and joint pain. Reduction in A1C may be slightly less than other agents as well.
Which diabetes medication would you add to Mr. AD existing therapy?
Here’s also a link to a helpful diabetes comparison table – https://diabetesed.net/wp-content/uploads/2018/01/ada-2018-meds-comparison-chart.jpg
- 30 medication mistakes PDF
- 18+ Page Drug Interaction PDF
- 10 Commandments of Polypharmacy Webinar based on my experiences in clinical practice


{kind=link}
I would add NOTHING. The data supporting <7% for HbA1c are not there. The UKPDS found no benefit over a median of 11 years for any macrovascular event. The VADT shows NO BENEFIT over 5.6 years with HbA1c 8.4% and 6.9% in the two groups. The ACCORD study showed NO BENEFIT over 3 years.
The ABSOLUTE difference to add SGLT2 is 0.6% to 1.6% over 3 years and 88% to 91% of the placebo patients did NOT have a CV event. I would not add these agents for a perceived and highly marketed CV reduction.
Cost considerations should ALWAYS be a consideration. It should be the cost to the HEALTH SYSTEM and not the co-pay or some manufacturer's coupon. The NNT in the empagliflozin and dapaglifozin studies are 63 and 167, respectively. the cost of these drugs are $5789 and $5904 per year (Goodrx.com). The studies with LOW p-values were 3 years long and used to hype these drugs. The cost for 3 years to prevent ONE event in these studies ranges from slightly more than $1 million to nearly $3 million. This is not a reasonable cost to PREVENT one event.
What is NOT given is the BP. I would be absolutely certain BP is well controlled. This is the best approach for this patient.
DPP 4
Interesting thoughts. What would you say is the healthcare costs of that one event though? Not only including hospitalization, but also potentially decreased qualoty of life? I’m not disagreeing that medications have a high cost, mostly just devil’s advocate
these therapies and urinary glucose loss is intresting and still i am thinking is that science is unable to find cure till now or it costly. thanks for information
Question: If he is already receiving an ACE-inhibitor/ thiazide diuretic combination for his hypertension management, what are some additional counseling points to be included in SGLT2 inhibitors plan ?
Answer : we risk dehydration and electrolyte disturbance , therefore we should point out the necessity of taking water and monitoring potassium ?