
Trazodone belongs to a class of drugs called serotonin antagonist and reuptake inhibitors (SARIs). Although trazodone is only FDA-approved for the treatment of major depressive disorder (MDD), it is most often used off-label to manage insomnia. What’s interesting about trazodone is the drug’s wide dosing range – with lower doses (25-150 mg) effectively managing insomnia and higher doses (up to 400-600 mg) treating MDD. At these different dosing ranges, trazodone hits different receptors with different affinities and is considered a dose-dependent multifunctional drug.
So what is the reason for this dose-dependent clinical response? It lies in trazodone’s pharmacodynamics!
Low Doses (25-150 mg)
At low doses, trazodone hits only the receptors for which it has the highest affinity: the 5-HT2A serotonergic, alpha-1 adrenergic, and histamine-1 receptors. It is well known that histamine plays a major role in sleep regulation, but it is also known that other neurotransmitter systems, including serotonin and norepinephrine, are involved in arousal mechanisms. Thus, simultaneous antagonism of these receptors produces hypnotic effects to induce and maintain sleep.
The figure below shows the relative binding affinities of trazodone for different receptors.
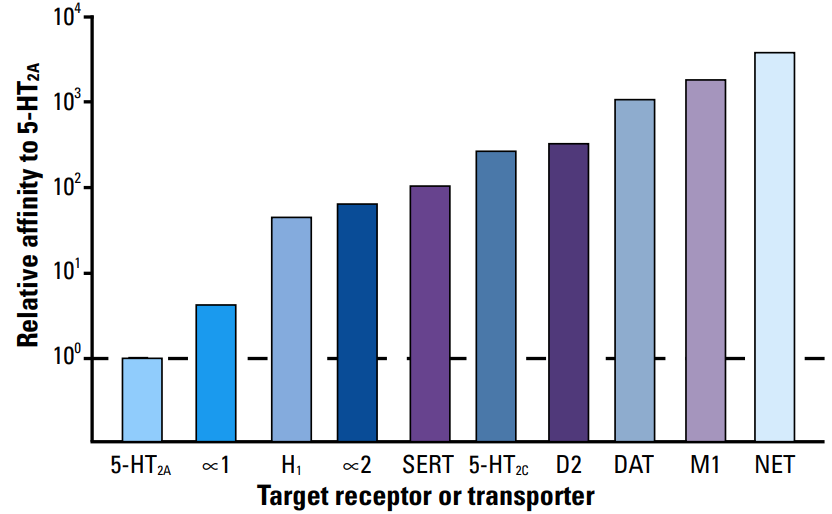
Figure obtained from Stahl SM. CNS Spectr. 2009;14(10):536-546.
High Doses (150-600 mg)
At higher doses, trazodone achieves antidepressant effects by saturating the serotonin receptors responsible for these effects. Trazodone simultaneously antagonizes the 5-HT2A and 5-HT2C receptors, inhibits the serotonin transporter (SERT), and weakly agonizes the 5-HT1A receptor to produce antidepressant and anxiolytic properties.
Clinical Response and Pharmacodynamic Action
| Clinical Response | Pharmacodynamic Action |
| Antidepressant Properties | 5-HT2A antagonism 5-HT2C antagonism SERT inhibition 5-HT1A partial agonism |
| Anxiolytic Effects | 5-HT2C antagonism |
| Insomnia Improvement | 5-HT2A antagonism H1 antagonism Alpha-1 receptor antagonism |
| Agitation Improvement | 5-HT2A antagonism Alpha-1 receptor antagonism |
| Anticholinergic Effects | M1 antagonism |
Table adapted from Fagiolini et al. Ann Gen Psychiatry. 2023;22(1):32.
Conclusion
It is evident that trazodone interacts with a variety of receptors to produce a wide range of clinical effects, earning the title of “multifunctional,” but it’s important to distinguish trazodone from other “dirty” drugs with off-target, undesired effects. Of course, trazodone’s complex pharmacodynamic profile isn’t without side effects, most commonly somnolence, dizziness, headache, and xerostomia. To a lesser extent, patients may experience orthostatic hypotension and priapism due to trazodone’s blockade of alpha-1 adrenergic receptors which occurs even at low doses. Compared to other antidepressants, trazodone has a better safety profile with a relatively lower risk of insomnia, anxiety, and sexual dysfunction. However, as with most serotonergic antidepressants, there is the risk of dose-dependent serotonin syndrome and suicidal thinking and behavior (Black Box Warning). Overall, trazodone has shown benefits for the treatment of insomnia when used at low doses.
This article was written by Kaitlyn Nichols, PharmD Candidate in collaboration with Eric Christianson, PharmD, BCPS, BCGP
- 30 medication mistakes PDF
- 18+ Page Drug Interaction PDF
- 10 Commandments of Polypharmacy Webinar based on my experiences in clinical practice
Popular Amazon Books






References:
- Fagiolini A, González-Pinto A, Miskowiak KW, Morgado P, Young AH, Vieta E. Role of trazodone in treatment of major depressive disorder: an update. Ann Gen Psychiatry. 2023;22(1):32.
- Jaffer KY, Chang T, Vanle B, et al. Trazodone for insomnia: A systematic review. Innov Clin Neurosci. 2017;14(7-8):24-34.
- Oggianu L, Di Dato G, Mangano G, et al. Estimation of brain receptor occupancy for trazodone immediate release and once a day formulations. Clin Transl Sci. 2022; 15(6):1417-1429.
- Settimo L, Taylor D. Evaluating the dose-dependent mechanism of action of trazodone by estimation of occupancies for different brain neurotransmitter targets. J Psychopharmacol. 2018;32(1):96-104.
- Stahl SM. Mechanism of action of trazodone: A multifunctional drug. CNS Spectr. 2009;14(10):536-546.


Do you feel trazodone for sleep is best dosed scheduled or as needed?
great review article on the use and MOA of Trazodone. It is often the second choice sleep agent in the geriatric population (OTC Melatonin being the preferred agent). Sleep disturbance can be a symptom of depression and anxiety, which I think is more common than the literature gives credit to. I think this maybe why I see so many residents admitted into SAR/LTC on more than one antidepressant by class agent. Sleep is so important in healing, behavior management and general well being of a patient and family members who provide care (ie spouce).
I really try emphasis the lowest effect dose in geriatric residents. Usually a low dose of 25-50mg qhs of Trazodone is very effective. Higher doses seem to cause more issues with BP and other side effect. Most geriatric residents are unable to tolerate more than 150mg of Trazodone without side effect issues.
Thanks for the comment!