
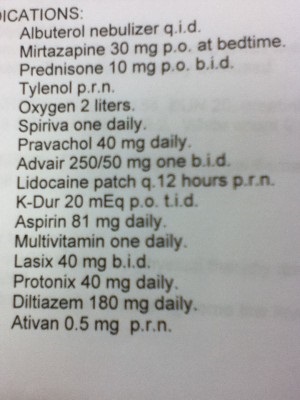
Reminder: For strategies to help minimize polypharmacy, subscribers have unlimited and free access to a webinar of the 10 Commandments of Polypharmacy – Please sign up! More content is in the works as well! Simply subscribe on the right hand side of the page (or down at the bottom of the page for mobile users). Here’s tonight’s med list!
Med List Review tonight! – Where I pick out a couple of points to prioritize, and you can help by adding in other things you’d like to investigate with the patient’s medications! I’m going to try to restrain myself tonight!
1. Pretty obvious to see from the meds that this patient has some significant respiratory issues. Between Advair, Spiriva, Albuterol, oxygen, and (likely) oral prednisone – this patient obviously struggles in that department. Always important to try to minimize systemic prednisone if possible, so would like to know if that’s a chronic dose or a short term burst. If chronic prednisone, osteoporosis amongst other things should be assessed/treated as appropriate (i.e. Vitamin D, Bisphosphonate).
2. Decent doses of Lasix/potassium, so I’d make sure the electrolytes/kidney function looks ok.
Plenty more to address – Thanks in advance for your ideas/comments!


With the Spiriva, Advair and 0xygen I would think the albuterol would be used as a “rescue” medication rather than “chronic QID”. While I’d like to see the patients K level I think the regimen could be simplified to 40 meq daily if K is within normal limits.,
Initially what’s the diagnosis? COPD ?
10mg BD for exacerbations will do nothing, 30mg OD for 7 days is standard.
Why the need to nebulise if they are already using an inhaler?, and if so why not on an abuterol MDI anyway?
I agree with the monitoring of [K], especially with Lasix, not even a banana would help that hypo. I see nebulised albuterol being used more frequently now for hyperkalaemia in medical wards, so we know how effective it can be in lowering [K].
Also check eGFR, if clearance is low, diltiazem won’t be helping the [K] levels either!.
http://www.ncbi.nlm.nih.gov/pubmed/1585928
If the albuterol is prn, then why is the K-Dur regular? running the risk of hyperkalaemia.
But the pharmacotherapy aside, if this patient does have COPD, I will always look at the whole patient, co-morbidities, bio-psycho-social factors too.
Addition of k-dur bid seems likley to counter the hypokalemic effect of Furosemaide, a standard regimen in managment of patients with chf. As you had pointed out use of albuterol concurrently on a regular basis would certainly cause major drop in potassium level, predisposing patient to disarythmia. Just a thought!
What dose is Tylenol? Also make sure nursing staff appropriately applying lidocaine patches with appropriate time off window, also would try to give 2nd prednisone dose as far from bedtime as possible 2 avoid insomnia (assuming remeron is 4 sleep)
I can see duplication already why give Albuterol and spriva at the same time and again a patient being given Ativan and pravachol at once it would be better to go for one