
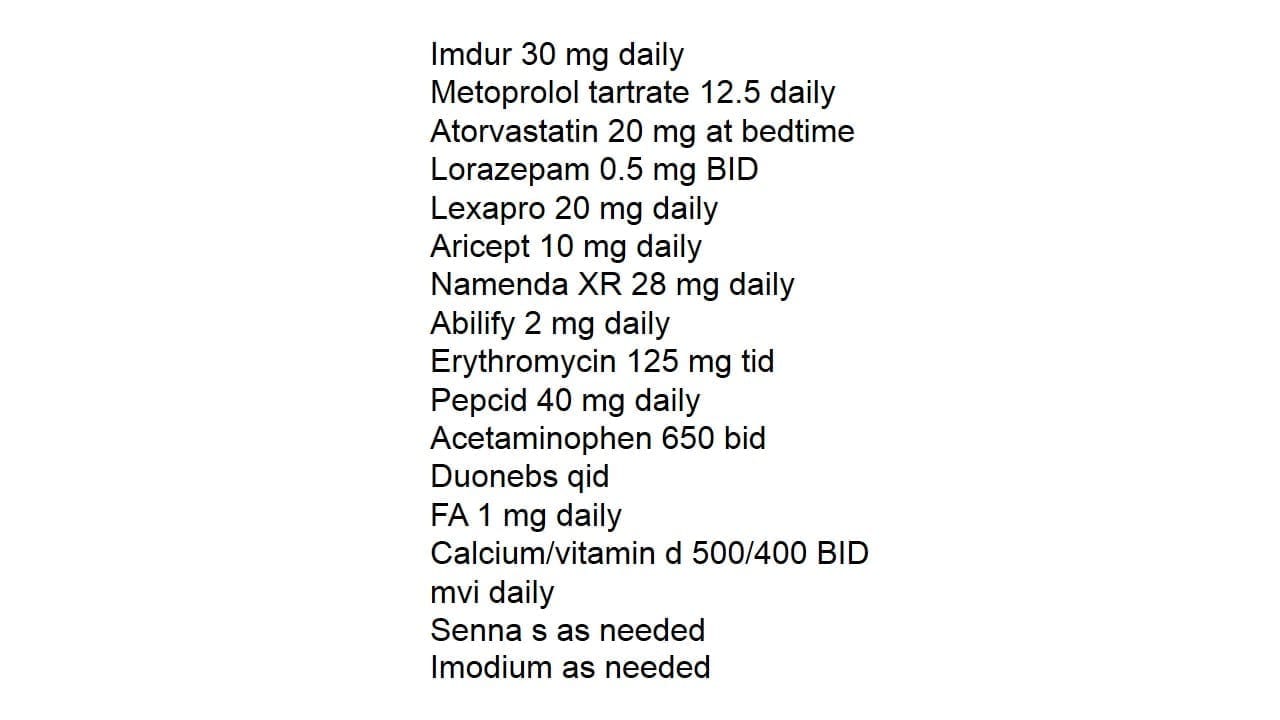
Tonight’s Medication List Review – First thing I want you to remember is whenever you see an order for Erythromycin, remember that it has a ton of drug interactions. So whenever we start, increase or decrease this medication, it can have ramifications on the concentrations of other medications.
I will highlight a couple possible interactions; Erythromycin can increase Abilify (aripiprazole) concentrations. Here’s a case where dose really makes a difference. While it is a legitimate concern, my concern would be much higher if this patient was on 30 mg of Abilify daily versus the current 2 mg order. Atorvastatin concentrations can also be increased due to the erythromycin and is something we need to monitor and be thinking about.
The other question I’d have with the erythromycin is why are we using it? I’ve seen this type of dosing before and would likely suspect chronic use not for an infection, but for GI motility. I’m not a big fan of using this due to all the interactions erythromycin can cause, but might have to be an option depending upon the case.
Check out the 30 medication mistakes that all healthcare professionals should be aware of! – A 6 page PDF free to subscribers – Click here for access!


Possible QT prolongation in this pt ??and erythromycin might possibly cause acute arrhythmia , possible contraindication .
This is a classic example of where MTM shines!!! A thorough understanding of the patient in the case is VERY important – med chart and SOAP notations help to categorize the situation. We get so used to seeing these combinations because for the average patient these drugs are doing EXACTLY what they are supposed to do with minimal negative effects. It’s when the patient is experiencing drug interactions issues, which most are simply from being on SO many potent agents, that we have to step back as the pharmacologists and classify issues that are presented as drug caused or illness caused.
The Erythromycin definitely has drug interactions and the potentiating or reducing effects have to be considered with the availability of alternative agents and what pathogen it’s being used to treat. The QT prolongation potential is higher with Azithro but the collective cardiac potential of the other agents on the list needs to be monitored.
The Abilify even at 2mg, effects Dopa and norepi along with every other chatecholamine. Both Dopa and Norepi are sympathomimetics that directly effect cardiac systems – remember we intentionally GIVE patients either dopa or norepi to maintain cardiac output. Lexapro is the s enantiomer of Celexa that selectively effects 5HT (cardiac/GI, manic/depression) but at higher or higher than needed doses will effect other chatecholamines . Aricept and Namenda affect acetylcholine and NMDA (depression/glutamine/pain mediation) and an Ativan booster. All potentially sedating, dampening agents so paradoxical hyperactivity is possible. These are things to keep in mind, but only act on if they present.
This patient is on meds that effect EVERY single chatecholamine , then cardiac meds and HMG-COa Inhibitor. If they are not experiencing ANY negative sides then leave it completely and monitor unless they can be switched from the antibiotic, even just for the sake of their GI flora.
If they are experiencing sides that can be moderated than these are some of the issues that can be explored. Were the psych meds added afterwards or were they the initial agents with cardiac/HMG-COa added afterwards? If it’s the latter, and no other psych meds can be offered that may reduce these effects (which may be possible since these are 2 of the best) then are the cardiac meds optimized for least sides and greatest effect? Psych meds affect glucose, cardiac and lipid metabolism and directly cause metabolic syndrome. Remember that if the patient is experiencing the negative sides, especially with psych agents, those negative sides ARE the PSYCH issues so it can be very disheartening! This class of agents, like epileptics etc, can actually worsen or even cause the symptom they are being used to treat!
For example, a psychiatrist places a manic patient with PTSD/OCD on aripiprazole 2mg and fluoxetine 10mg and will titrate appropriately. After 2 weeks the patient anxiety is worse and can’t sleep so the doc slightly ups the fluoxetine and this continues. We as MTM PharmD’s can help by reminding the psychiatrist to run labs at dosing titrations as per guidelines to rule out metabolic syndrome/neuroleptic malignant syndrome and MOST COMMONLY Serotonin Syndrome. All 3 of these syndromes, especially early on, can MIMIC MANIA, depression, etc. Again the drugs, especially fluoxetine with it’s prolonged half life and accumulation abilities, can actually cause the syndrome the med is designed to alleviate and this can be identified by RUNNING LABS. In house labs are MUCH cheaper than correcting the effects later.
This patient is an excellent case of – if there’s nothing to fix leave it, if there is an issue there’s plenty of room for adjustment and monitoring here because ALL of the above mentioned agents interact with each other- either synergistically or negatively!
When an interaction presents ask:
What has been tried in the past? Patients, age, comorbid disease, sex, symptoms, etc? What are the diagnoses? When did they present? How is this patient’s CrCl, BUN (dehydrated), LDH, weight, input./output, glucose, ALT/AST, etc, etc – acid balance, age, etc.
As MTM PharmD’s we are the extra set of ‘pharmacology specialty’ trained eyes that can ADD to the assessments of these types of patients.
Thank you Eric, again for a fantastic case! Exceptional case truly!!
No problem, great comment!
great reply. learned alot
The dose of erythromycin suggests its use as a prokinetic agent. Do they need it? If the anticholinergic side-effects of the other therapies require a stimulant, perhaps bisacodyl could be given a trial.
Why are we treating a patient on Namenda XR and Aricept with atorvastatin? What is the rationale? I would have the atorvastatin discontinued.