
In this article, we provide the latest acne treatment guidelines as well as clinical pearls of the most commonly used agents.
Acne is a very common disease that plagues teens and young adults. Acne can persist into later adulthood, but the incidence is far less frequent. Around 85% of people are affected by acne at some point during their teenage years1, with about 12% of adult women also suffering from acne beyond teenage years.3 Prevalence of acne in the United States is more than 50 million people, resulting in over $3 billion of expenditures and loss of productivity per year.2
There is limited knowledge surrounding molecular and cellular mechanisms and the immunopathogenesis of acne. The pathophysiology of acne scarring is also not well understood. According to the American Academy of Dermatology, acne vulgaris is thought to be a multifaceted process involving several factors:
- Follicular hyperkeratinization
- Microbial colonization of P. acnes
- Excessive sebum production
- Inflammatory mechanisms
- Neuroendocrine regulation
- Diet
- Genetic predisposition
Currently, there are not any specific recommendations from clinical guidelines regarding dietary management for the resolution and prevention of acne. Studies suggest that diets with a high glycemic index may contribute to the development of acne. Patients may consider cutting out and limiting different types of food to assess for possible trigger foods.1
To date, there is not a universally accepted grading and classification tool used to assess acne severity. Providers often develop their own method based on clinical characteristics and their effect on the quality of life to drive therapeutic decisions and evaluate treatment response. In practice, treatment algorithms are often anecdotal in nature due to a lack of high-quality studies and data. Below, is the acne treatment guidelines (algorithm) taken from the 2016 clinical guidelines from the American Academy of Dermatology.1
Acne treatment guidelines algorithm:
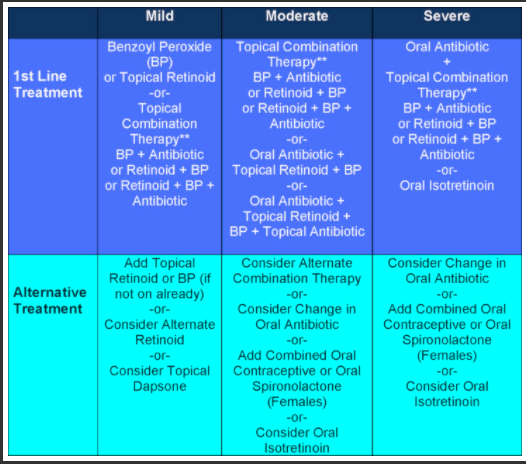
Taken from American Academy of Dermatology Guidelines of care for the management of acne vulgaris; 2016
Clinical Considerations of Potential Treatments:
Benzoyl Peroxide (BP): Safe, effective, and available OTC. BP is effective in preventing microbial resistance and should be used in patients on topical or oral antibiotics. Side effects – Contact dermatitis, erythema, & peeling, Avoid contact with eyes and mucous membranes, may bleach hair and fabric
Topical Retinoids: Includes adapalene, tretinoin, and terazotene. Increased risk of photosensitivity. Often side effects limit retinoid use. Side effects – dryness, peeling, erythema, and irritation
- Adapalene – considered most tolerable and can be used at same time as BP.
- Tretinoin – should not be administered at the same time as BP, as BP may inactivate the retinoid.
- Terazotene – Most associated with side effects but may be most effective.
- Pregnancy category X.
Topical antibiotics: Erythromycin and clindamycin. Effective treatments but need to be used with BP or Retinoids to prevent bacterial resistance.
- Clindamycin: Wash face with mild soap and allow to completely dry prior to administration. Side effects include skin irritation, avoid contact with eyes and mucous membranes.
- Erythromycin: side effects include dry or scaly skin, irritation, itching, or stinging.
Oral antibiotics: Used in moderate-severe cases of acne. Duration of therapy should be shortest possible – typically 3-4 months. Use antibiotics in conjunction with retinoid or retinoid/BP. These topical agents will then be used as maintenance therapy long-term.
- Tetracyclines (doxycycline & minocycline) are preferred agents. Side effect: Photosensitivity, GI upset, dizziness, tinnitus, and pigmentation of skin, mucous membranes, and teeth.
- Macrolides can be effective but should be restricted to use in patients unable to be on tetracyclines (pregnancy, < 8 years of age, allergy). Side effects: GI upset, increased risk of QT prolongation, ototoxicity.
- TMP/SMX, penicillins, and cephalosporins are sometimes used, however supporting data is limited and these agents should be restricted to patients unable to take preferred agents above.
Oral contraceptives (COC, Females): COCs are effective in treating inflammatory acne in females through the anti-androgenic effects. Risks vs benefits need to be considered on an individual basis because estrogen-containing contraceptives increased risk of VTE, stroke, and MI. There are also questions regarding low estrogen therapy’s effect on bone mass in adolescent patients. COCs are FDA approved for females at least 14 years old but should be avoided within 2 years of starting menses. Contraindicated in: pregnancy, breastfeeding, active breast cancer, 35 years old and heavy (15 cigarettes/day) smoker, and HTN > 160/100 mmHg.
Spironolactone (Females): Provides antiandrogenic effects that have shown significantly improved outcomes in the treatment of acne. Currently, it is FDA off-label usage with doses ranging from 50-200mg daily. Typically, well-tolerated with side effects being dose-related. Side effects – Diuresis, menstrual irregularities, breast tenderness, headache, dizziness, fatigue.
Isotretinoin: Indicated for moderate, treatment-resistant, or severe acne, or acne that is causing physical scarring or psychosocial distress. LFTs and a lipid panel should be monitored at baseline and periodically throughout treatment. For optimum absorption, isotretinoin should be taken with food (Absorica formulations can be taken with or without food). Side effects – Alopecia, photosensitivity, dermatitis, arthralgia, musculoskeletal pain, dry mouth, dry eyes, and hypertriglyceridemia. Avoid additional vitamin A supplementation (retinoids) while on therapy.
- Highly teratogenic – Patient must comply with iPledge Program in conjunction with provider and pharmacist to start and continue treatment with isotretinoin. Patients who can become pregnant need 2 reliable forms of contraception. Patient-independent birth control like long-acting reversible contraception should be considered. Unfortunately, due to non-compliance with the abstinence and/or contraceptive efforts, there are still approximately 150 isotretinoin-exposed pregnancies in the United States each year.
Hopefully this provides you some valuable information with regards to the acne treatment guidelines and a few clinical pearls you can use in your practice!
Article written by Joseph Nelson in collaboration with Eric Christianson, PharmD BCPS, BCGP
- 30 medication mistakes PDF
- 18+ Page Drug Interaction PDF
- 10 Commandments of Polypharmacy Webinar based on my experiences in clinical practice
Study Materials and Resources For Healthcare Professionals and Students – Amazon Books
References:
1) Zaenglein AL, Pathy AL, Schlosser BJ, et al. Guidelines of care for the management of acne vulgaris. Journal of the American Academy of Dermatology. 2016;74(5):945-973. doi:10.1016/j.jaad.2015.12.037
2) Bhate K, Williams HC. Epidemiology of acne vulgaris. Br J Dermatol. 2013;168(3):474-485. doi:10.1111/bjd.12149
3) Goulden V, Stables GI, Cunliffe WJ. Prevalence of facial acne in adults. J Am Acad Dermatol. 1999;41(4):577-580.
*IBM Micromedex was used to reference administration, side effects, etc. of treatments.*


0 Comments